FAQ
-
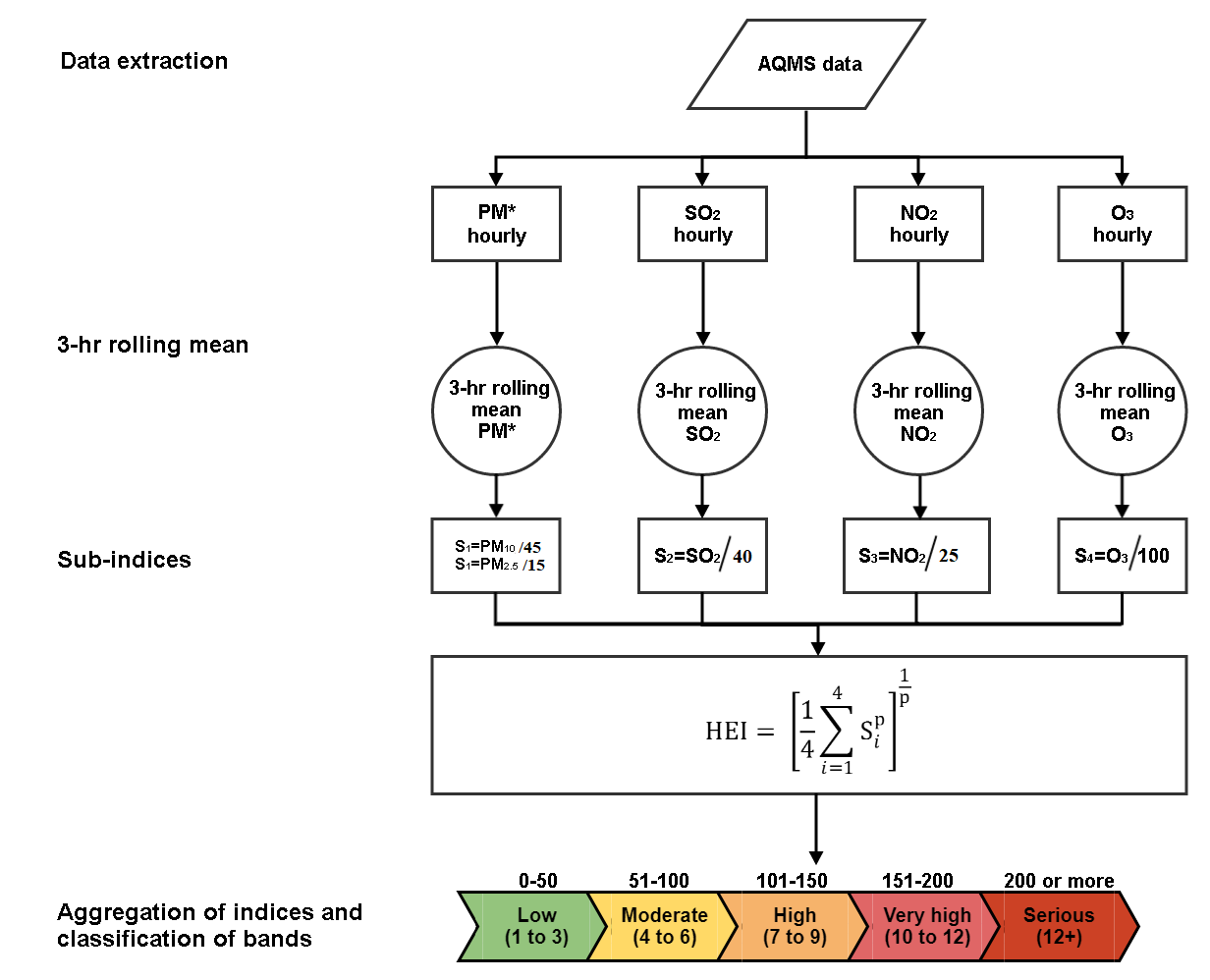
For a given station, each hourly pollutant concentration is converted into standardized values:

Pollutant concentration is defined as the mean of the past three hours readings. If two or more readings are missing then the sub-index si is regarded as missing.
A sub-index value of 100 means the pollutant is at a concentration equal to the corresponding the short-term World Health Organization Air Quality Guidelines (WHO AQG) limit.
WHO AQG limits (2021 guidelines) are: 15 µg/m3 for PM2.5; 45 µg/m3 for PM10; 40 µg/m3 for SO2; 25 µg/m3 for NO2; 100 µg/m3 for O3.
After we divide the standard of each pollutant we have a standardized set of values that we can then aggregate them by:
The HEI is calculated and reported only when all 4 sub-indices are not missing otherwise the HEI is reported as missing (NA). In the calculations of the HEI, we take the higher of the two sub-indices of PM10 and PM2.5.
The overall HEI of Hong Kong is calculated based on the median of HEI among all urban rooftop stations.
-
Avoidable harm refers to the amount of adverse health effects due to air pollution in our population. Since air pollution is mainly anthropogenic and could be prevented through strong political will and environmental management, therefore the associated serious adverse health effects are clearly avoidable. We estimated the amount of avoidable harm using a few observable health effects, including all non-accidental causes of mortality (premature deaths), hospitalization (hospital bed-days) and outpatient consultations (doctor visits) for cardiopulmonary diseases.
We used (i) the total numbers of these health outcomes in the population in 2013-2014, multiplied by (ii) locally determined risk estimates which quantify the total numbers of bad health outcomes for each unit increase in air pollutant concentration, and then by (iii) the number of units of air pollutant concentration exceeding the World Health Organization (WHO) annual Air Quality Guidelines (AQG). Finally, we combined the effects of each of the four criteria air pollutants (PM10, SO2, NO2 and O3) by taking account of the partial correlations between them. We calculated exposure in terms of air pollutant concentration using 61% roadside and 39% urban rooftop pollutant levels. Our current estimation method is quite conservative since the best available local scientific estimates that are applied to calculate adverse effects are based on short-term effect estimates, which are often much smaller than long-term effect estimates.
-
We calculated the overall health-related community costs of air pollution using the amount of adverse health effects caused by air pollution which we have so far been able to measure in our population. These costs can be categorized as the direct costs of health care; the indirect costs due to lost productivity and the intangible costs attributable to pain and suffering (defined as “loss of healthy life value”).
The bad health outcomes include non-accidental causes of mortality (premature deaths), hospitalization (hospital bed-days) and outpatient consultations (doctor visits) for cardiopulmonary diseases. However, there are many other health problems now known to be attributable to air pollution which have not yet been quantified in Hong Kong. These include a wide spectrum of harm to pregnant mothers, infants and people with diabetes. Therefore our current estimation of economic loss is likely to be an underestimation of the real economic burden due to air pollution, but it is evidence-based and provides a conservative translation of health impacts to a monetary value to support policy decision making.
In our economic appraisal the direct health care costs due to the bad health outcomes attributable to air pollution include public and private hospital admissions (valued as bed days used), public out-patient consultations at general, specialist and accident and emergency clinics for cardiovascular and respiratory diseases (valued as cost of visits plus travel costs) and primary care doctor visits (valued as cost of visits plus travel).
Indirect costs are the value of lost productivity due to work absence caused by sickness or early death for those of working age (15 to 64 years) and time lost from work due to hospital admissions and doctor visits. All losses were adjusted for current employment rates and valued as gender-specific median daily salaries.
Intangible losses for lives lost due to air pollution were based on the average value of a lost life in Hong Kong. This was estimated from population surveys of the willingness-to-pay to avoid the loss of one statistical life (HK$10 million or US$1.28 million). This is a conservative estimate, comparable to the range of US$0.4 to $9.7 million reported from Europe, Australia, New Zealand, US and Canada. To this we added the value of avoiding hospital admissions and coughing episodes which were over and above the costs of treatment. These values were also taken from local surveys of the willingness to pay to avoid the bad outcomes.
-
A clear day is a day in which all five criteria pollutants (i.e. PM2.5, PM10, SO2, NO2 and O3) at all fifteen urban rooftop stations complied with the short-term World Health Organization Air Quality Guidelines (WHO AQG). We have used green colour to represent a clear day and grey colour to represent a polluted day. The use of fifteen rooftop monitoring stations is based on the Environmental Protection Department’s method for counting the number of exceedance days in Hong Kong. This counting method does not include roadside monitoring stations so that exposure is still under-represented. Nevertheless, our counting based on WHO AQG provides a more valid method of risk communication to the public than by any method of counting based on other lax limit values.
Air Pollutant Short-term WHO AQG (µg/m³) No. of allowed exceedance per year in WHO AQG PM25 15 3.00 PM10 45 3.00 SO2 40 0.00 NO2 25 0.00 O3 100 0.00